Beyond Wachter: 1% for the 99% was originally published on DigitalHealth.net
Beyond Wachter: 1% for the 99%
Ewan Davis and Tony Shannon say there is a lot to like about the Wachter Review, but identify some worrying gaps between its approach and NHS policy. They call for an open platform and a challenge fund to secure digital transformation for all, and not just for the exemplars.
####
As the NHS looks forward to another/perpetual winter, it has the Wachter Review to read. This is the outcome of the review of NHS IT (actually acute IT) that health secretary Jeremy Hunt asked US ‘digital doctor’ Robert Wachter to undertake last November.
We broadly welcome Watcher’s recommendations, but they don’t go far enough. So far, their main impact has been to encourage Hunt and NHS England to announce a programme of investment focused on a few “exemplar” trusts, which Hunt has described as an ‘Ivy League’ for others to aspire to.
In combination, we don’t see any sign of the radically different approach that is required if digital technology is going to enable the radical transformation the NHS requires.
The good points
Complex, not complicated: Healthcare has been misunderstood as a complicated endeavor for too long. Complicated machines, such as aircraft, are engineered to have a predictable relationship between the switches in the cockpit and the connected component parts.
A typical hospital is a good deal more complex than that. It is much better understood as an ecosystem than a machine. The Wachter Review, thankfully, acknowledges that healthcare is a complex “adaptive system”, in which evolution rather than revolution reigns supreme, and says that digitising healthcare should be understood in that context.
IG and training: Digitising healthcare for the right reasons and at the right speed, working with patients to promote an effective balance between data sharing and effective privacy controls, and developing a professional workforce properly trained in informatics good practice are further key principles that it sets out that are well worth advocating.
Smart recommendations: The ten related recommendations are mostly smart, too. They Include a push for trained clinical informaticians with resource and authority at board level, along with a push for local networks to share learning, and a call for the NHS to join the international push for greater interoperability.
Missing pieces and policy gaps
Hospital centric mindset: The forward looking ‘Five Year Forward View’, issued by NHS England chief executive Simon Stevens to try and close a £30 billion gap between NHS funding and demand by 2020-21, rightly focuses on the need for integration across health and social care communities.
Indeed, it goes further in calling for the creation of accountable care organisations (which it calls primary and acute care systems). The focus of Wachter and NHS England seems to be on a few acute hospitals and the new programme of global and national digital exemplars.
Lack of patient centred thinking/care: The Forward View also recognises the importance of engaging patients and their informal care networks and putting these at the centre of care. Watcher has little to say about patient engagement and the exemplar programme’s focus on hospitals with 20th century megasuites does little to create the digital ecosystem required to enable innovative patient faces apps and services.
Platform approach: It’s widely recognised that open platforms have been key to digital transformation in other sectors and that the creation of such platforms is essential if we want to see digital transformation in health and care. Yet there is nothing in Watcher or in subsequent announcements that gives support to open platform approaches.
Given that the well-respected global consultancy McKinsey http://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/how-healthcare-systems-can-become-digital-health-leaders tells us that ‘Open Innovation Platforms’ have the potential to save more than 11% of total healthcare costs, and that this view supported by Accenture, which describes platforms as creating a “(R)evolution” in healthcare”, this seems to be both a surprising and unforgivable omission.
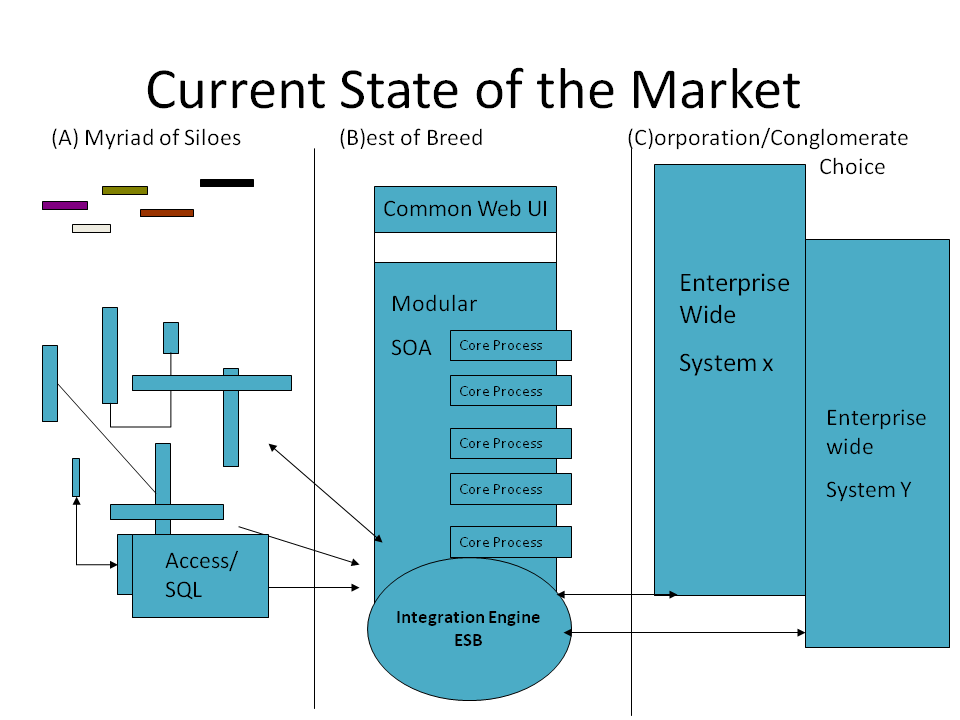
So what are platforms and what do we mean a platform approach?
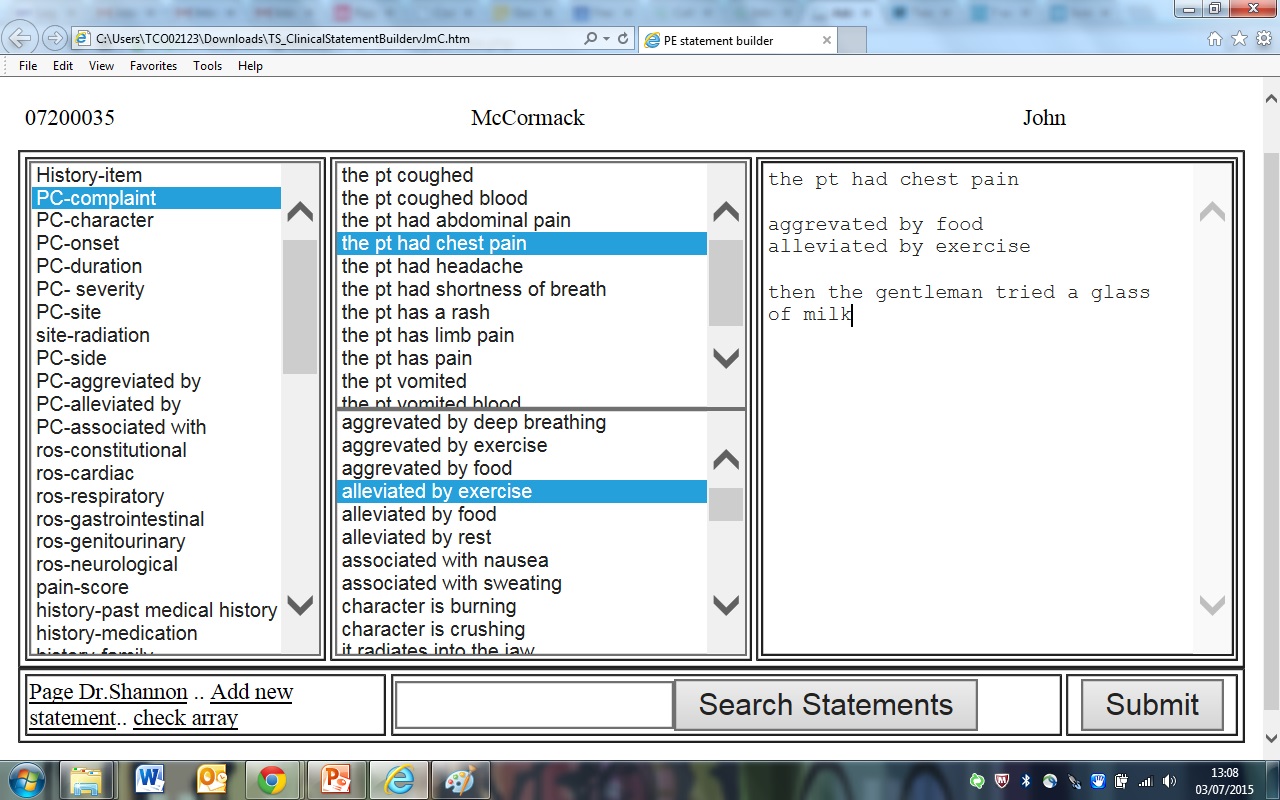
A platform provides an information infrastructure; a set of shared services based on common standards, on which developers can build applications that work together. By using standard components, and providing services that offload common tasks from application developers, they enable those developers to concentrate on the unique features of their application, delivering more quickly and providing a spur to innovation.
Attempts to create a platform for health go back 20 years. Initial efforts by suppliers focused on attempts to own the platform but, while some still seek that monopoly, there is now a growing consensus that only an open platform approach can succeed in healthcare.
In the end, governments, healthcare systems and market participants will not accept monopolistic/proprietary ownership of the platform. By an open platform, we don’t just mean some proprietary systems with some open application programming interfaces, but rather implementations that:
- Are based on open standards
- Share common information models
- Support application portability
- Are federatable
- Are vendor and technology neutral
- Store data in a common open format.
These definitions align with the forward thinking ‘Digital Supplier Standard’ now emerging from Gov.uk https://www.gov.uk/government/consultations/supplier-standard-for-digital-and-technology-service-providers/supplier-standard-for-digital-and-technology-service-providers By taking this approach vendor lock-in is eliminated, as one platform implementation is easily replaced with another and applications are easily portable across different implementations.
The use of a common open data format ensures vendors work towards the goal of an integrated patient centred record architecture, meaning data does not get locked into a proprietary format and is easily shared, simplifying interoperability and cross-border flows.
Open platforms go further than closed platforms in that they facilitate international cooperation while moving the market away from vendor lock-in and towards a market for services that add real value. There are a number of approaches that might support such an open platform but we believe that the most promising is, openEHR.
This both meets these principles and is already being successfully implemented on a large scale to enable integrated patient centred care elsewhere in the world; perhaps most notably in Moscow. http://www.woodcote-consulting.com/moscow-ehealth-a-model-for-the-uk/
A call to action: 1% for the 99%
Even if McKinsey’s view of the potential of open platforms and their estimated savings to the NHS of £14 billion (11% of the annual £130 billion NHS spend) are grossly overstated, the potential is clearly such that it is amazing that that open platforms don’t feature at all in the NHS’s latest plans.
We recognise that open platforms in healthcare will take time to embed. However, the technology on offer is already mature and has the support of a global community of clinicians and vendors.
Therefore, our challenge to the NHS is to try something different to investing in the “usual suspects” and to shift just 1% of the £4 billion planned investment in NHS IT over the next five years to proactively stimulate innovation.
We think that £40 million should be used to create an ‘Open Platforms Challenge Fund’ open to small and medium sized enterprises partnering with health and social care providers. Open it up, and let’s discover what this group can do.
To the skeptics, we’d suggest a look at the results delivered by the recent very small investment by the NHS in initiatives like Apperta’s Code4Health Programme and the Ripple Open Source Initiative. To the visionaries, we’d invite you to join us on our journey, one we believe is destined to change healthcare and bring it into the 21st Century at last.
We want 1% for the 99% beyond the Ivy League…
About the authors:
Ewan Davis has worked in digital health since 1981, and now works for Woodcote Consulting. woodcote-consulting.com He works closely with the HANDI Health CIC, a not-for-profit organisation established to help the health and care app community, and writes regular columns for Digital Health on open source, open platform, and other IT issues. @Woodcote_Ewan
Dr Tony Shannon has worked in frontline clinical practice for 20 years, with ten of those as a consultant in emergency medicine in the NHS, where he has also held the CCIO roles for Leeds Teaching Hospitals NHS Foundation Trust and Leeds City, leading on the Leeds Care Record. www.leedscarerecord.org. He is the director of Frectal www.frectal.com and of the Ripple Foundation, which has been set up to foster a community of health and social care pioneers in England by collaborating around an open Integrated Care Record platform. www.rippleosi.org @frectally
Published on DigitalHealth.net on 12th October 2016